Psychology of a CrisisPsychology of a Crisis
2019 Update
CS 290397-E
2 CERC: Psychology of a Crisis
CERC: Psychology of a Crisis
Explanations of figures for accessibility found in the Appendix: Accessible Explanation of Figures on page 16.
This chapter will introduce:
Four Ways People Process Information During a Crisis
Mental States in a Crisis
Behaviors in a Crisis
Negative Vicarious Rehearsal
Addressing Psychology in the CERC Rhythm
Crises, emergencies, and disasters happen. Disasters
are different from personal and family emergencies,
and not just because they are larger in scale. Disasters
that take a toll on human life are characterized by
change, high levels of uncertainty, and complexity.
1
In a crisis, affected people take in information,
process information, and act on information
differently than they would during non-crisis
times.
2,3
People or groups may exaggerate their
communication responses. They may revert to more
basic or instinctive fight-or-flight reasoning.
Effective communication during a crisis is not
an attempt at mass mental therapy, nor is it a magic
potion that fixes all problems. Nonetheless, to reduce
the psychological impact of a crisis, the public should
feel empowered to take actions that will reduce their
risk of harm.
This chapter will briefly describe how people
process information differently during a crisis, the
mental states and behaviors that tend to emerge in
crises, how psychological effects are different in each
phase of a crisis, and how to communicate to best
reach people during these changing states of mind.
3 CERC: Psychology of a Crisis
Four Ways People Process Information
during a Crisis
By understanding how people take in information during a crisis state, we can better plan to communicate
with them. During a crisis:
We simplify messages.
4
Under intense stress and possible information
overload, we tend to miss the nuances of health
and safety messages by doing the following:
■ Not fully hearing information because of our
inability to juggle multiple facts during a crisis.
■ Not remembering as much of the information as
we normally could.
■ Misinterpreting confusing action messages.
To cope, many of us may not attempt a logical and
reasoned approach to decision making. Instead, we
may rely on habits and long-held practices. We might
follow bad examples set by others.
Use simple messages.
We hold on to current beliefs.
5,6
Crisis communication sometimes requires asking
people to do something that seems counterintuitive,
such as evacuating even when the weather
looks calm.
Changing our beliefs during a crisis or emergency
may be difficult. Beliefs are often held very strongly
and not easily altered. We tend not to seek evidence
that contradicts beliefs we already hold.
We also tend to exploit any conflicting or
unclear messages about a subject by interpreting
it as consistent with existing beliefs. For example,
we might tell ourselves, “I believe that my house is a
safe place.” Before an impending hurricane, however,
experts may recommend that we evacuate from
an insecure location and take shelter in a building
that is stronger and safer. Although the action
advised is actually for us to evacuate our house to
seek a safer shelter, we can easily misinterpret the
recommendation to match our current beliefs. We
might say, “My home is strong and safe. I’ve always
been secure in my home. When we left last time, the
hurricane went north of us anyway. I’ll just stay here.”
Faced with new risks in an emergency, we may
have to rely on experts with whom we have little
or no experience. Often, reputable experts disagree
regarding the level of threat, risks, and appropriate
advice. The tendency of experts to offer opposing
views leaves many of us with increased uncertainty
and fear. We may be more likely to take advice from a
trusted source with which we are familiar, even if this
source does not have emergency-related expertise
and provides inaccurate information.
Messages should come from a credible source.
4 CERC: Psychology of a Crisis
We look for additional information and opinions.
7, 8
We remember what we see and tend to believe what
we’ve experienced. During crises, we want messages
confirmed before taking action. You may find that
you or other individuals are likely to do the following:
■ Change television channels to see if the same
warning is being repeated elsewhere.
■ Try to call friends and family to see if others have
heard the same messages.
■ Turn to a known and credible local leader for
advice.
■ Check multiple social media channels to see what
our contacts are saying.
In cases where evacuation is recommended, we tend
to watch to see if our neighbors are evacuating before
we make our decision. This confirmation first—before
we take action—is very common in a crisis.
Use consistent messages.
We believe the first message.
9
During a crisis, the speed of a response can be an
important factor in reducing harm. In the absence
of information, we may begin to speculate and fill
in the blanks. This often results in rumors. The first
message to reach us may be the accepted message,
even though more accurate information may follow.
When new, perhaps more complete information
becomes available, we compare it to the first
messages we heard.
Because of the ways we process information while
under stress, when communicating with someone
facing a crisis or disaster, messages should be
simple, credible, and consistent. Speed is also very
important when communicating in an emergency. An
effective message must do the following:
■ Be repeated.
■ Come from multiple credible sources.
■ Be specific to the emergency being experienced.
■ Offer a positive course of action that can
be executed.
Release accurate messages as soon as possible.
5 CERC: Psychology of a Crisis
Mental States in a Crisis
During a disaster, people may experience a wide
range of emotions. Psychological barriers can
interfere with cooperation and response from the
public. Crisis communicators should expect certain
patterns, as described below, and understand that
these patterns affect communication.
There are a number of psychological barriers
that could interfere with cooperation and response
from the public. A communicator can mitigate
many of the following reactions by acknowledging
these feelings in words, expressing empathy, and
being honest.
Uncertainty
Unfortunately, there are more questions than
answers during a crisis, especially in the beginning.
At that time, the full magnitude of the crisis, the
cause of the disaster, and the actions that people
can take to protect themselves may be unclear.
This uncertainty will challenge even the greatest
communicator.
To reduce their anxiety, people seek out
information to determine their options and confirm
or disconfirm their beliefs. They may choose a
familiar source of information over a less familiar
source, regardless of the accuracy of the provided
information.
7
They may discount information that is
distressing or overwhelming.
Many communicators and leaders have been
taught to sound confident even when they are
uncertain. While this may inspire trust, there is a
potential for overconfidence, which can backfire. It is
important to remember that an over-reassured public
isn’t the goal. You want people to be concerned,
remain vigilant, and take all the right precautions.
Acknowledge uncertainty. Acknowledge and
express empathy for your audience’s uncertainty
and share with them the process you are using to
get more information about the evolving situation.
This will help people to manage their anxiety. Use
statements such as, “I can’t tell you today what’s
causing people in our town to die so suddenly, but I
can tell you what we’re doing to find out. Here’s the
first step…”
Tell them
■ What you know.
■ What you don’t know.
■ What process you are using to get answers.
Although we can hope for certain outcomes, we
often cannot promise that they will occur. Instead of
offering a promise outside of your absolute control,
such as “we’re going to catch the evil people who
did this,” promise something you can be sure that
response officials will do, such as “we’re going to
throw everything we have at catching the bad guys,
or stopping the spread of disease, or preventing
further flood damage.”
Former New York City Mayor Rudolph Giuliani
cautioned, “Promise only when you’re positive. This
rule sounds so obvious that I wouldn’t mention it
unless I saw leaders break it on a regular basis.”
10
A
danger early in a crisis, especially if you’re responsible
for fixing the problem, is to promise an outcome
outside your control. Never make a promise, no
matter how heartfelt, unless it’s in your absolute
power to deliver.

6 CERC: Psychology of a Crisis
Fear, Anxiety, and Dread
In a crisis, people in your community may feel
fear, anxiety, confusion, and intense dread. As
communicators, our job is not to make these feelings
go away. Instead, you could acknowledge them in a
statement of empathy. You can use a statement like,
“we’ve never faced anything like this before in our
community and it can be frightening.”
Fear is an important psychological consideration
in the response to a threat. Bear in mind the
following aspects of fear:
■ In some cases, a perceived threat can motivate and
help people take desired actions.
■ In other cases, fear of the unknown or fear of
uncertainty may be the most debilitating of the
psychological responses to disasters and prevent
people from taking action.
■ When people are afraid, and do not have adequate
information, they may react in inappropriate ways
to avoid the threat.
Communicators can help by portraying an accurate
assessment of the level of danger and providing action
messages so that affected people do not feel helpless.
Hopelessness and Helplessness
Avoiding hopelessness and helplessness is a
vital communication objective during a crisis.
Hopelessness is the feeling that nothing can be
done by anyone to make the situation better. People
may accept that a threat is real, but that threat may
loom so large that they feel the situation is hopeless.
Helplessness is the feeling that people have that
they, themselves, have no power to improve their
situation or protect themselves. If a person feels
helpless to protect him- or herself, he or she may
withdraw mentally or physically.
According to psychological research, if
community members let their feelings of fear,
anxiety, confusion, and dread grow unchecked
during a crisis, they will most likely begin to feel
hopeless or helpless.
11
If this happens, community
members will be less motivated and less able to take
actions that could help themselves.
Instead of trying to eliminate a community’s
emotional responses to the crisis, help community
members manage their negative feelings by
setting them on a course of action. Taking an
action during a crisis can help to restore a sense of
control and overcome feelings of hopelessness and
helplessness.
11
Helping the public feel empowered
and in control of at least some parts of their lives may
also reduce fear.
As much as possible, advise people to take
actions that are constructive and directly relate to the
crisis they’re facing. These actions may be symbolic,
such as putting up a flag or preparatory, such as
donating blood or creating a family check-in plan.
7 CERC: Psychology of a Crisis
Denial
Denial refers to the act of refusing to acknowledge
either imminent harm or harm that has already
occurred. Denial occurs for a variety of reasons:
■ People may not have received enough information
to recognize the threat.
■ They may assume the situation is not as bad as
it really is because they have not heard the most
recent warnings, didn’t understand what they were
told, or only heard part of a message.
■ They may have received messages about a threat
but not received action messages on how people
should respond to the threat.
■ They may receive and understand the message,
but behave as if the danger is not as great
as they are being told. For example, people
may get tired of evacuating for threats that
prove harmless, which can cause people to
deny the seriousness of future threats.
When people doubt a threat is real, they may seek
further confirmation. With some communities, this
confirmation may involve additional factors, such as
the following:
■ A need to consult community leaders or experts
for specific opinions.
■ The desire to first know how others are responding.
■ The possibility that the warning message of the
threat is so far outside the person’s experience that
he or she simply can’t make sense of it—or just
chooses to ignore it.
Denial can, at least in part, be prevented or
addressed with clear, consistent communication
from a trusted source. If your audience receives and
understands a consistent message from multiple
trusted sources, they will be more likely to believe
that message and act on it.
What about Panic?
Contrary to what you may see in the movies, people
seldom act completely irrationally during a crisis.
12
During an emergency, people absorb and act on
information differently from nonemergency situations.
This is due, in part, to the fight-or-flight mechanism.
The natural drive to take some action in response
to a threat is sometime described as the fight-or-
flight response. Emergencies create threats to our
health and safety that can create severe anxiety,
stress, and the need to do something. Adrenaline, a
primary stress hormone, is activated in threatening
situations. This hormone produces several responses,
including increased heart rate, narrowed blood
vessels, and expanded air passages. In general, these
responses enhance people’s physical capacity to
respond to a threatening situation. One response
is to flee the threat. If fleeing is not an option
or is exhausted as a strategy, a fight response is
activated.
13
You cannot predict whether someone will
choose fight-or-flight in a given situation.
These rational reactions to a crisis, particularly
when at the extreme ends of fight-or-flight, are
often described erroneously as “panic” by the media.
Response officials may be concerned that people
will collectively “panic” by disregarding official
instructions and creating chaos, particularly in public
places. This is also unlikely to occur.
If response officials describe survival behaviors as
“panic,” they will alienate their audience. Almost no
one believes he or she is panicking because people
understand the rational thought process behind
their actions, even if that rationality is hidden to
spectators. Instead, officials should acknowledge
people’s desire to take protective steps, redirect
them to actions they can take, and explain why the
unwanted behavior is potentially harmful to them or
the community. Officials can appeal to people’s sense
of community to help them resist unwanted actions
focused on individual protection.
In addition, a lack of information or conflicting
information from authorities is likely to create
heightened anxiety and emotional distress. If you start
hedging or hiding the bad news, you increase the risk
of a confused, angry, and uncooperative public.
8 CERC: Psychology of a Crisis
Media Coverage of Crisis and Potential Psychological Effects
As we will see later in this chapter, most of us tend to
have stronger psychological and emotional reactions
to a crisis if it’s manmade or imposed.
14
These types
of crises also tend to have increased media exposure.
The media will often show repeated negative images,
such as the following:
■ People who are dying or in distress.
■ People who lack food and water.
■ Animals that have been abandoned, hurt, or
covered in oil.
■ Landscapes, such as collapsed buildings, flooded
homes, or oil floating on top of water.
Those who are indirectly affected by the crisis
through media exposure may personalize the event
or see themselves as potential victims. For example,
on September 11, 2001, adults watched an average
of 8.1 hours of television coverage, and children
watched an average of 3.0 hours.
14
Several studies
show that the amount of time spent watching TV
coverage and the graphic content of the attacks
on September 11 was associated with increased
post-traumatic stress disorder (PTSD) and clinical
depression symptoms.
15,16,17
This was even true
for those far away from disaster sites. In addition,
those who were directly affected by the attacks and
watched more television coverage had higher rates
of PTSD symptoms and depression than those who
did not.
As you are planning your communication
strategy, remember that even those people not
directly affected by an emergency may have
substantial psychological effects. Communication
targeted at them will also need to use sound crisis
and emergency risk communication principles.
Behaviors in a Crisis
Proper crisis communication can address a variety of
potentially harmful behaviors during a crisis. Although
it may be difficult to measure the impact, using good
communication to persuade people to avoid negative
behaviors during a crisis will save lives, prevent
injuries, and lessen the misery people experience.
Some of these negative behaviors are listed here, with
advice on communication strategies to address them.
Seeking Special Treatment
Some people will attempt to bypass official channels
to get special treatment or access to what they want
during a crisis. For instance, in Richard Preston’s book
Demon in the Freezer, an account of the eradication
of smallpox, neighbors and friends approached the
wife of a prominent government smallpox researcher
asking for help to obtain smallpox vaccine in case
of a bioterrorist attack with smallpox.
18
The vaccine

9 CERC: Psychology of a Crisis
was not available for these people through official
channels, so they reached out to someone with
influence, who they thought could assist them.
This behavior may result from the following:
■ A person’s sense of privilege.
■ A belief that officials cannot guarantee the
person’s well-being.
■ An inflated need to be in control.
■ A lack of awareness of available resources.
Whatever the cause, seeking special treatment
can be damaging to the harmony and recovery of
the community. If there is a perception that favored
people get special help, it invites anger among
community members and chaos when resources are
made available.
Some supplies or treatments may first be
given to priority groups who are either especially
vulnerable to the disaster, such as children and
elderly people, or whose safety is critical to an
effective response, such as healthcare workers.
The term “priority groups” may confuse some people,
who may be unclear about what criteria are used to
define priority and may assume they are important
enough to be in a priority group. To avoid this,
communicators can discuss those groups who have
the greatest need for treatment without referring to
them as “priority groups.”
Good communication can reduce some of these
reactions. The more honest and open government
officials are about resources, the better odds officials
have of reducing the urge among people in the
community to seek special treatment. The following
communication strategies can help communicators
persuade the public to avoid seeking special treatment:
■ Explain what resources are available.
■ Explain why some resources are not available.
■ Explain that limited supplies are being used for
people with the greatest need.
■ Explain who the people are with the greatest need.
■ Describe reasonable actions that people can take, so
that they do not focus on things they cannot have.
■ Keep open records of who receives what and when.
Remember, both people directly affected by the
crisis and those who anticipate being affected by
the crisis need enough information to help them
manage anxiety and avoid behaviors that may divide
the community.
Negative Vicarious Rehearsal
In an emergency, many communication and
response activities are focused on audiences who
were directly affected, such as survivors, people
who were exposed, and people who had the
potential to be exposed. However, these targeted
messages will also reach people who do not need
to take immediate action. Some of these unaffected
observers may mentally rehearse the crisis as if they
are experiencing it and practice the courses of action
presented to them.
In many cases, this mental rehearsal can help to
prepare people for the actions they should take in an
emergency. This may reduce anxiety and uncertainty.
As a communicator, you may encourage this type
of mental rehearsal by asking an audience not yet
affected by an emergency to create an emergency
plan of action according to your recommendations.
Other times, spectators farther away from the
emergency may be much more critical about the
value of your recommendations because they have
more time to decide their chosen course of action.
In some cases, they may reject the proposed course
of action and choose another. If a person rejects an
action, it may be harder for that person to take that
action in the future. For example, if people hear a
story about a search and rescue effort for someone
lost in the wilderness they may mentally rehearse
how they would act in a similar situation. If they plan
out creating an elaborate shelter, starting a fire and
finding food, instead of finding a simple shelter
and water and waiting for rescue, then those are
the actions they might choose to take in the event
that they do find themselves lost in the wilderness.
This would decrease their survival chances because
they would waste their energy and resources on less
important actions.
People practicing negative vicarious rehearsal
might decide that they are at the same risk as
those directly affected by the emergency and need
the recommended remedy, such as a visit to an
emergency room or a vaccination. These people,
sometimes referred to as the “worried well,” may
heavily tax response resources by requesting medical
treatment they do not need. For example, during
10 CERC: Psychology of a Crisis
the 2011 earthquake, tsunami, and radiation disaster
in Japan, people who lived on the west coast of the
United States and Canada began to worry about
radiation exposure coming across the ocean. Because
people very close to the danger in Japan had been
advised to take potassium iodide (KI) to mitigate
effects of radiation, some people in North America
thought they should take KI too. In fact, when
unneeded, KI has dangerous side effects and should
not be used.
Communicators can help to address the effects
of negative vicarious rehearsal by creating simple
action steps that can be taken by the people not
directly affected by an emergency. Simple actions
in an emergency will give people a better sense of
control and will help to motivate them to stay tuned
to your messages. During the Japan emergency,
communicators related to people on the West Coast
what they could do to help people in Japan; what
they could do to learn more about actual levels of
radiation reaching the United States; and directed
them to fact sheets about when KI was and was
not necessary. “Let your friends know KI can be
dangerous when not needed” became a new action
people could take.
When communicators create messages, they
are likely to segment their target audience into
groups who need to take different types of action.
The challenge is to convince people unaffected
by the emergency to delay taking the same action
recommended to people directly affected unless
their circumstances change. Create alternative action
messages for those people who are vicariously
experiencing the threat, but who should not take
the action currently being recommended to those
directly affected.
Stigmatization
Stigmatization can affect a product, an animal, a
place, and an identifiable group of people. It occurs
when the risk is not present in the stigmatized
minority group but people associate the risk with
that group. Stigmatization is especially common in
disease pandemics.
If a population becomes stigmatized, members of
this group may experience emotional pain from the
stress and anxiety of social avoidance and rejection.
Stigmatized people may be denied access to health
care, education, housing, and employment. They may
even be victims of physical violence.
Crisis communicators must be aware of the
possibility that, although unintentional and
unwarranted, segments of their community could
be shunned because some perceive them as being
identified with the problem. This could have both
economic and psychological impact on the well-
being of members of the community and should
be challenged immediately. This stigmatization can
occur without any scientific basis. It can come not
only from individuals, but entire nations. During the
first avian influenza outbreak in Hong Kong during
1997–98 and during the first West Nile virus outbreak
in New York City in 1999, the policies of some other
nations banned the movement of people or animals,
despite the absence of clear science calling for those
measures.
Communication professionals must help to
counter potential stigmatization during a disaster.
You should be cautious about images you share
repeatedly and understand that constant portrayal
of a segment of the population in images may
contribute to stigmatization. For instance, if the
images accompanying a news story about a disaster
consistently show members of a particular ethnic
group, this may reinforce the idea that the disaster
is associated with members of that ethnic group. If
stigmatizing statements or behaviors appear, public
health officials must offset this with accurate risk
information that people can understand, and speak
out against the negative behavior.
It is important to remember that even if
stigmatization decreases through the beginning
of the crisis lifecycle, the stigma may return in the
resolution phase. As misery and anger turns to fault-
finding and blame, the group of people perceived to
be responsible for the disaster could be stigmatized
once again. Keep this in mind when creating your
communication strategy.

11 CERC: Psychology of a Crisis
Harmful Actions Brought About by
Crisis-Related Psychological Issues
Without communication from a source that is
trusted by the audience to lessen the psychological
impact, negative emotions may lead to harmful
individual or group behaviors. These behaviors may
affect the public’s safety by slowing the speed,
quality, and appropriateness of a crisis response and
recovery. Crisis-related psychological issues may lead
to further loss of life, health, safety, and property.
Harmful actions may include the following:
■ Misallocating treatments based on demand rather
than medical need.
■ Accusations of providing preferential treatment
and bias in providing aid.
■ Creating and spreading damaging rumors and
hoaxes directed at people or products.
■ Offering unfounded predictions of greater
devastation.
■ Encouraging an unfair distrust of response
organizations.
■ Attempting bribery for scarce or rationed
treatments and resources.
■ Depending on special relationships to ensure
considerations based on desire, not need.
People in a crisis tend to have more unexplained
physical symptoms. Stress caused by a crisis situation
will give some people physical symptoms, such
as headaches, muscle aches, stomach upsets, and
low-grade fevers.
19
In emergencies involving disease
outbreaks, these symptoms could confound the
effort to identify those people who need immediate
care versus those who need only limited treatment or
limited access to medication.
Positive Responses following a Crisis
Crises do not only create negative emotions and
behaviors. Positive responses might include coping,
altruism, relief, and elation at surviving the disaster.
Feelings of excitement, greater self-worth, strength,
and growth may come from the experience. Often
a crisis results in changes in the way the future is
viewed, including a new understanding of risks and
new ways to manage them.
How quickly the crisis is resolved and the degree
to which resources are made available will make a
difference. Many of these positive feelings associated
with a successful crisis outcome depend on
effective management and communication. Positive
responses may include the following:
■ Relief and elation.
■ Sense of strength and empowerment.
■ New understanding of risk and risk management.
■ New resources and skills for risk management.
■ Renewed sense of community.
■ Opportunities for growth and renewal.
12 CERC: Psychology of a Crisis
Risk Perception
20,21
Not all risks are perceived equally by an audience.
Risk perception can be thought of as a combination
of hazard, the technical or scientific measure of a
risk, and outrage, the emotions that the risk evokes.
Risk perception is not about numbers alone.
Don’t dismiss outrage. The mistake some
officials make is to measure the magnitude of the
crisis only based on how many people are physically
hurt or how much property is destroyed. Remember
that we must also measure the catastrophe
in another way: the level of emotional trauma
associated with it.
As a communicator, expect greater public outrage
and more demands for information if what causes the
risk is manmade and, especially, if it’s intentional and
targeted. Unfairly distributed, unfamiliar, catastrophic,
and immoral events create long-lasting mental health
effects that lead to anger, frustration, helplessness,
fear, and a desire for revenge. A wide body of research
exists on issues surrounding risk communication,
but the following explains how some risks are more
accepted than others:
■ Voluntary versus involuntary: Voluntary
risks are more readily accepted than imposed
risks. Example: elective knee surgery v. emergency
appendectomy.
■ Personally controlled versus controlled by
others: Risks controlled by the individual or
community are more readily accepted than risks
outside the individual’s or community’s control.
Example: choosing to house a nuclear reactor in the
community v. having a nuclear reactor built in your
community against your wishes.
■ Familiar versus exotic: Familiar risks are more
readily accepted than unfamiliar risks. Example:
seasonal influenza v. a new respiratory illness.
■ Natural origin versus manmade: Risks
generated by nature are better tolerated than risks
generated by man or institution. Example: a natural
disaster v. an oil spill.
■ Reversible versus permanent: Reversible
risk is better tolerated than risk perceived to be
irreversible. Example: having a broken leg v. having
an amputated leg.
■ Endemic versus epidemic: Illnesses, injuries, and
deaths spread over time at a predictable rate are
better tolerated than illnesses, injuries, and deaths
grouped by time and location. Example: seasonal
influenza v. pertussis (whooping cough) outbreak.
■ Fairly distributed versus unfairly distributed:
Risks that do not appear to single out a group,
population, or individual are better tolerated than
risks that are perceived to be targeted. Example:
water pollution that is citywide v. water pollution in a
minority neighborhood.
■ Generated by trusted institution versus
mistrusted institution: Risks generated by a
trusted institution are better tolerated than risks
that are generated by a mistrusted institution.
Example: air pollution by coal plant that is a longtime
area employer v. air pollution by new and unknown
company.
■ Adults versus children: Risks that affect adults
are better tolerated than risks that affect children.
Example: lead paint in an office building v. lead paint
in a school.
■ Understood benefit versus questionable
benefit: Risks with well-understood potential
benefit and the reduction of well-understood
harm are better tolerated than risks with little or no
perceived benefit or reduction of harm. Example:
chemotherapy for cancer is a risk with a well-
understood benefit.
■ Statistical versus anecdotal: Statistical risks
for populations are better tolerated than risks
represented by individuals. Example: an anecdote
shared with a person or community, even if it is
explained to be a “one in a million” event, can be
more damaging than a statistical risk of one in 10,000
presented as a number.
13 CERC: Psychology of a Crisis
Addressing Psychology in
the CERC Rhythm
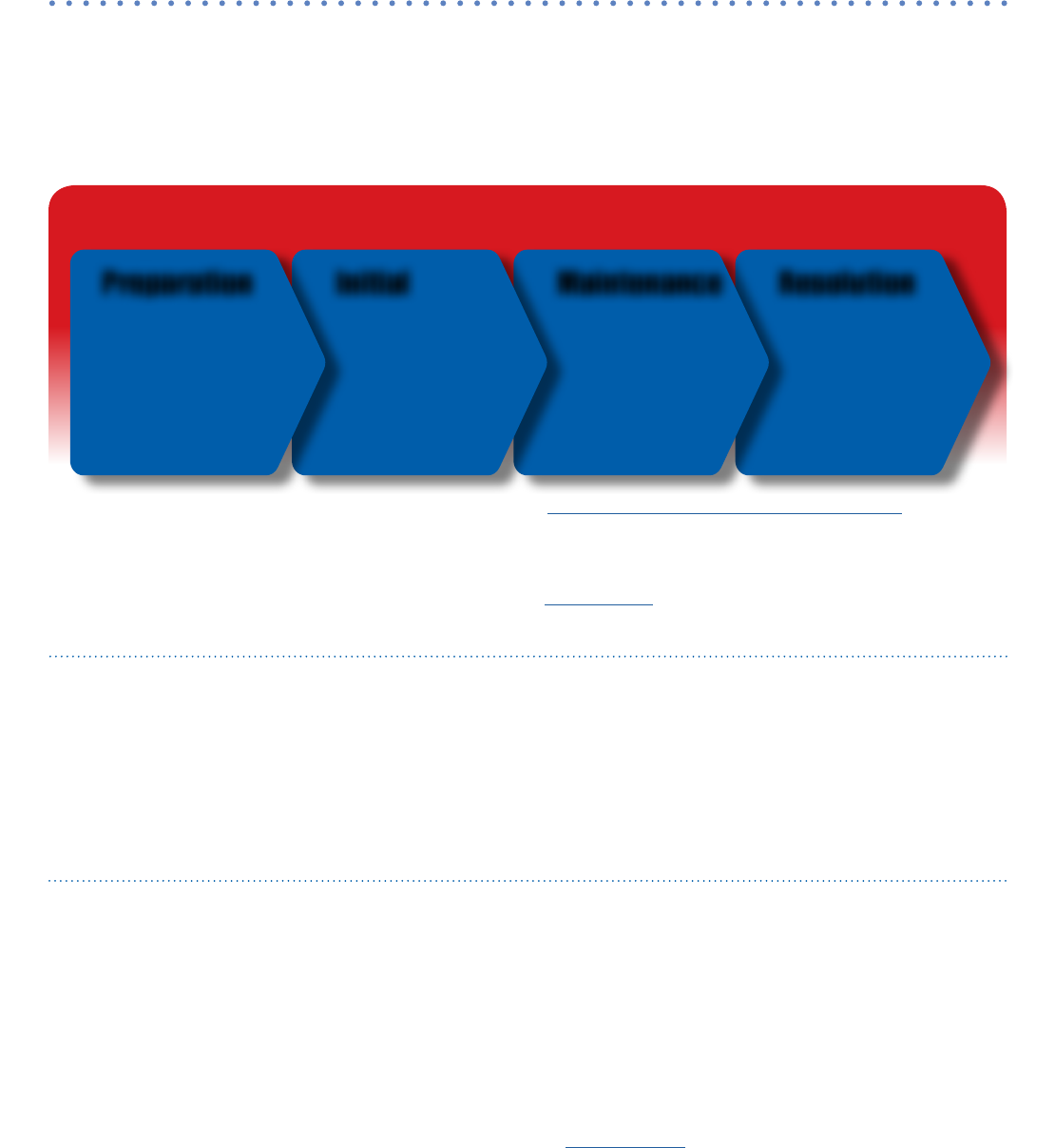
The CERC Rhythm graphic shows the four phases of a crisis. Accessible explanation of figure in Appendix, page 16.
In addition to the principles of risk communication
described, such as expressing empathy and being
respectful, it’s important to consider how the situation
changes during each phase of a crisis and how risk
communication can be applied during each phase.
Although these phases were discussed in our
introduction, it’s helpful to have a more in-depth
picture of each category.
Preparation
Important information and assumptions are set
during the pre-crisis stage even before a crisis occurs.
Develop plans and establish open communication
during this phase.
Provide an open and honest flow of
information to the public: Generally, more harm is
done by officials trying to avoid panic by withholding
information or over-reassuring the public, than is
done by the public acting irrationally in a crisis. Pre-
crisis planning should assume that you will establish
an open and honest flow of information.
Initial
During this stage of acute danger, the priority
for all is basic safety and survival. Most people
respond appropriately to protect their lives and
the lives of others.
22
To reduce the threat, they
create spontaneous efforts to cooperate with
others. However, some may behave in disorganized
ways and may not respond as expected. The more
stress felt in a crisis, the greater the impact on the
individual. Important causes of stress include the
following:
■ Threat to life and encounters with death.
■ Feelings of powerlessness and helplessness.
■ Personal loss and dislocation, such as being
separated from loved ones or home.
■ Feelings of being responsible, such as telling
oneself “I should be doing more.”
■ Feelings of facing an inescapable threat.
■ Feelings of facing malevolence from others, such
as deliberate efforts that cause harm.
During the initial phase, the following CERC concepts
are important. These concepts are explained further
in spokesperson.
■ Don’t over-reassure.
■ Acknowledge uncertainty.
■ Emphasize that a process is in place to
learn more.
■ Be consistent in providing messages.
Engage Community • Empower Decision-Making • Evaluate
The CERC Rhythm
Preparation ResolutionMaintenanceInitial
■ Draft and test
messages
■ Developpartnerships
■ Create plans
■ Determine approval
process
■ Express empathy
■ Explain risks
■ Promote action
■ Describe response
efforts
■ Explain ongoing risks
■ Segment audiences
■ Provide background
information
■ Address rumors
■ Motivate vigilance
■ Discuss lessons
learned
■ Revise plan
14 CERC: Psychology of a Crisis
Put the good news in secondary clauses
For example, “it’s too soon to say we’re out of the woods, even though we haven’t seen a new anthrax case
in X days.” The main clause indicates that you are taking the situation seriously and that you are responding
aggressively. The secondary clause includes the reassuring information without over-reassuring.
Maintenance
During this phase, the crisis magnitude, the concept
of personal risk, and the initial steps toward recovery
and resolution are in motion. Emotional reactions vary
and will depend on perceptions about the risk and
the stresses people experienced or anticipated. At first
people may appear to be elated, despite surrounding
destruction or death, because they are relieved they
survived. However, as the maintenance phase evolves,
people may experience varied emotional states,
including numbness, denial, flashbacks, grief, anger,
despair, guilt, and hopelessness.
The longer the maintenance phase lasts, the
greater these reactions. Once basic survival needs are
met, other needs for emotional balance and self-
control emerge. People often become frustrated and
let down if they are unable to return to more normal
conditions. Early selfless responses to the emergency
may fall away and be replaced by negative emotions
and blame.
The following CERC principles apply to the
maintenance phase and are further explained in the
chapter on spokesperson:
■ Acknowledge fears.
■ Express wishes.
■ Give people things to do.
■ Acknowledge shared misery.
■ Give anticipatory guidance (foreshadow).
Resolution
When the emergency is no longer on the front
page, those who have been most severely affected
will continue to have significant emotional needs.
Emotional symptoms may present as physical health
symptoms such as sleep disturbance, indigestion, or
fatigue. They may cause difficulties with interpersonal
relationships at home and work. At this point,
organized external support often starts to erode
and the realities of loss, bureaucratic controls, and
permanent life changes come crashing down.
To maintain trust and credibility during the
resolution phase, keep the expressed commitments
from the initial phase. Failures or mistakes should be
acknowledged and carefully explained.
15 CERC: Psychology of a Crisis
References
1. Seeger MW, Sellnow TL, Ulmer RR. Communication and organizational crisis. Westport (CT): Praeger; 2003.
2. Covello VT, Peters RG, Wojtecki JG, Hyde RC. Risk communication, the West Nile virus epidemic, and
bioterrorism: responding to the communication challenges posed by the intentional or unintentional
release of a pathogen in an urban setting. J Urban Health 2001;78(2):382–391.
3. Glik DC. Risk communication for public health emergencies. Annu Rev Public Health 2007;28: 33–54.
4. Hill D. Why they buy. Across the Board 2003;40(6):27–33.
5. Andreasen AR. Marketing social change: changing behavior to promote health, social development, and
the environment. San Francisco: Jossey-Bass Publishers;1995.
6. Brehm SS, Kassin S, Fein S. Social psychology. 6th ed.Boston: Houghton Mifflin Co.;2005.
7. Brashers DE. Communication and uncertainty management. J Commun 2001;51(3):477–497.
8. Sellnow TL, Ulmer RR, Seeger MW, Littlefield RS. Effective risk communication: A message-centered
approach. New York: Springer Science+Business Media, LLC;2009.
9. Solso RL. Cognitive psychology. 6th ed. Boston:Allyn and Bacon;2001.
10. Giuliani, R. Leadership. New York: Miramax; 2005. p. 164–165.
11. Benight CC, Bandura A. Social cognitive theory of posttraumatic recovery: The role of perceived self-
efficacy. Behaviour research and therapy, 42(10), 1129–1148;2004.
12. Clarke, L. The problem of panic in disaster response. [online]. 2003. [cited 2019 Feb]. Available from URL:
http://www.centerforhealthsecurity.org/our-work/events/2003_public-as-asset/Transcripts/index.html#clarke.
13. Sellnow TL, Seeger MW. Theorizing crisis communication. Malden (MA): Wiley-Blackwell; 2013. p. 7.
14. Novac A. Traumatic stress and human behavior. Psychiatric Times [online] 2001 Apr [cited 2019 Feb]; 18(4).
Available from URL: http://www.psychiatrictimes.com/dissociative-identity-disorder/traumatic-stress-and-
human-behavior.
15. Ahern J, Galea S, Resnick H, Kilpatrick D, et al. (2002). Television images and psychological symptoms after
the September 11 terrorist attacks. Psychiatry, 65(12), 289–300;2002.
16. Schuster MA, Stein BD, Jaycox LH, Collins RL, Marshall GN, Elliott MN, Berry SH. A national survey of stress
reactions after the September 11, 2001, terrorist attacks. New Engl J Med, 345(20), 1507–1512;2001.
17. Schlenger WE, Caddell JM, Ebert L, Jordan BK, Rourke KM, Wilson D, Kulka RA. Psychological reactions to
terrorist attacks: findings from the national study of americans’ reactions to September 11. J Am Med,
288(5), 581–588;2002.
18. Preston R. The demon in the freezer. New York: Random House; 2003.
19. Stuart JA, Ursano RJ, Fullerton CS, Norwood AE, Murray K. Belief in exposure to terrorist agents: reported
exposure to nerve or mustard gas by Gulf War veterans. Journal of nervous and mental disease, 191(7),
431–436; 2003.
20. Cohn V. Reporting on risk: getting it right in an age of risk. Washington (DC): The Media Institute; 1990.
21. Covello V. Communicating Radiation Risks. Crisis communications for emergency responders. EPA
Document 402-F-07-008 [online]. 2007. [cited 2019 Feb]. Available from URL: http://tinyurl.com/6lva2sk
22. U.S. Department of Veterans Affairs. National Center for PTSD. Phases of traumatic stress reactions in a
disaster. Impact phase [online]. 2018 Jan. [cited 2019 Feb]. Available from URL: https://www.ptsd.va.gov/
professional/treat/type/index.asp.
16 CERC: Psychology of a Crisis
Resources
■ American Psychological Association. The effects of trauma do not have to last a lifetime [online]. 2004 Jan 16.
[cited 2019 Feb]. Available from URL: http://www.apa.org/research/action/ptsd.aspx.
■ DeWolfe, DJ. Mental health response to mass violence and terrorism: a field guide. DHHS Pub. SMA 4025.
Rockville (MD): Substance Abuse and Mental Health Services Administration [online]. 2005. [cited 2019 Feb].
Available from URL: https://store.samhsa.gov/product/Mental-Health-Response-to-Mass-Violence-and-
Terrorism-A-Field-Guide/SMA05-4025
■ DiGiovanni C Jr. Domestic terrorism with chemical or biological agents: psychiatric aspects. Am J Psychiatry
1999 Oct;156(10):1500–5.
■ Everly GS Jr, Mitchell JT. America under attack: the “10 commandments” of responding to mass terrorist
attacks. Int J Emerg Ment Health 2001 Summer;3(3):133–5.
■ Krug EG, Kresnow M, Peddicord JP, Dahlberg LL, Powell KE, Crosby AE, et al. Suicide after natural disasters. N
Engl J Med 1998 Feb 5;338(6), 373–378.
■ Reynolds BJ. When the facts are just not enough: credibly communicating about risk is riskier when emotions
run high and time is short. Toxicol Appl Pharmacol 2011 Jul 15;254(2):206–14.
■ Schuster MA, Stein BD, Jaycox LH, Collins RL, Marshall GN, Elliott MN, et al. A national survey of stress reactions
after the September 11, 2001 terrorist attacks. N Engl J Med 2001;345(20), 1507–1512.
■ Sandman, Peter M. The risk communication website. Risk = hazard + outrage [online]. 2004 [cited 2019 Feb].
Available from URL: http://www.psandman.com/index.htm.
■ Tinker, Tim L, and Elaine Vaughan. Risk and crisis communications:best practices for government agencies
and non-profit organizations. McLean, Va: Booz, Allen, Hamilton, 2010. Print.
■ U. S. Department of Veterans Affairs. National Center for PTSD. Psychological first aid: field operations guide
[online]. 2006. [cited 2019 Feb]. Available from URL: https://www.ptsd.va.gov/professional/treat/type/psych_
firstaid_manual.asp.
■ U.S. National Library of Medicine. Current bibliographies in medicine 2000–2007. Health risk communication
[online]. 2000 Oct. [cited 2019 Feb]. Available from URL: https://www.nlm.nih.gov/archive/20061214/pubs/
cbm/health_risk_communication.html
Appendix: Accessible Explanation of Figures
The CERC Rhythm (page 13): Crisis communication
needs and activities evolve through four phases
in every emergency. The first phase is preparation.
During preparation communicators should
draft and test messages, develop partnerships,
create communication plans, and determine the
approval process for sending out information in an
emergency. The second phase is the initial phase.
During the initial phase of a crisis communicators
should express empathy, explain risks, promote
action, and describe response efforts. During the
third phase, maintenance, communicators need
to explain ongoing risks and will have more time
to segment audiences, providing background
information, and addressing rumors. The final phase,
resolution, requires communicators to motivate the
public to stay vigilant and communicators should
discuss lessons learned and revise communication
plans for future emergencies. Throughout all phases,
CERC encourages communicators to engage
communities, empower community members to
make decisions that impact their health, and evaluate
communication efforts.
